Minimally invasive mesh repair for all hernia types — inguinal, umbilical, and incisional — with faster recovery and lower recurrence rates than open surgery.

A hernia happens when an organ or a bit of fatty tissue pushes through a weak point in the muscle wall around it. The groin, belly button and old surgical scars are the most common places for this to happen. The four main types are the inguinal hernia (groin), umbilical hernia (belly button), incisional hernia (through a previous surgical scar) and femoral hernia (upper inner thigh).
Hernias do not go away on their own. Left alone, they tend to get bigger and more uncomfortable. In some cases the trapped tissue loses its blood supply — a condition called strangulation — which is a medical emergency that needs surgery right away.
Keyhole (laparoscopic) repair is now the preferred approach for most hernias. The surgeon works through three small cuts, guided by a camera. A synthetic mesh is placed over the weak spot and stitched in place, reinforcing the wall so the hernia cannot come back. Recurrence rates are below 2 to 3 percent.
Book a consultation with Dr. Prashanth J V today.
Book Consultation 📞 +91 93533 16175The entire procedure is performed under general anaesthesia and takes 45 to 90 minutes depending on the hernia type and complexity. You are completely comfortable throughout.
You will be under general anaesthesia, so you are completely asleep and comfortable. The technique used depends on the hernia: TEP (Totally Extraperitoneal) stays outside the abdominal cavity, while TAPP (Trans-Abdominal Pre-Peritoneal) briefly enters it for a wider view.
Three incisions, each 5 to 12 mm, are made in the abdomen. One is at the navel for the camera, and two are for the surgical instruments. The laparoscope sends a magnified, high-definition view to a screen in the operating theatre.
The protruding tissue is gently guided back into the abdominal cavity. The hernia sac is separated from the surrounding structures and either removed or tucked away, preparing the area cleanly for mesh placement.
A lightweight, body-compatible mesh is laid over the defect and secured with small tacks or sutures. The mesh acts as a scaffold; over the following weeks, the body's own tissue grows into it to create a strong, lasting repair.
The port sites are closed with dissolving stitches and small dressings. Most patients are walking around within a few hours and are ready to go home the same day or after one overnight stay.
Mild soreness around the cuts. Walking is encouraged the same day. Start with liquids and move to soft foods as you feel ready.
Pain managed with tablets. Short walks, light household tasks and personal care are fine. Stitches dissolve by themselves.
Most people return to desk work and can drive again. A follow-up visit checks wound healing and confirms the mesh is settling correctly.
Gradual return to the gym, sport and heavier lifting. The mesh is fully integrated into the wall and the long-term repair is holding well.
Hundreds of laparoscopic hernia repairs performed using both TEP and TAPP techniques, with consistently low recurrence and complication rates.
Whether your hernia calls for TEP, TAPP or open repair, the choice is made based on your specific anatomy, hernia size and history. Not a one-size-fits-all decision.
Every consultation covers your options honestly. You leave knowing exactly what the surgery involves, what recovery looks like and what results to expect.
 Gallbladder Surgery
Gallbladder Surgery Appendicectomy
Appendicectomy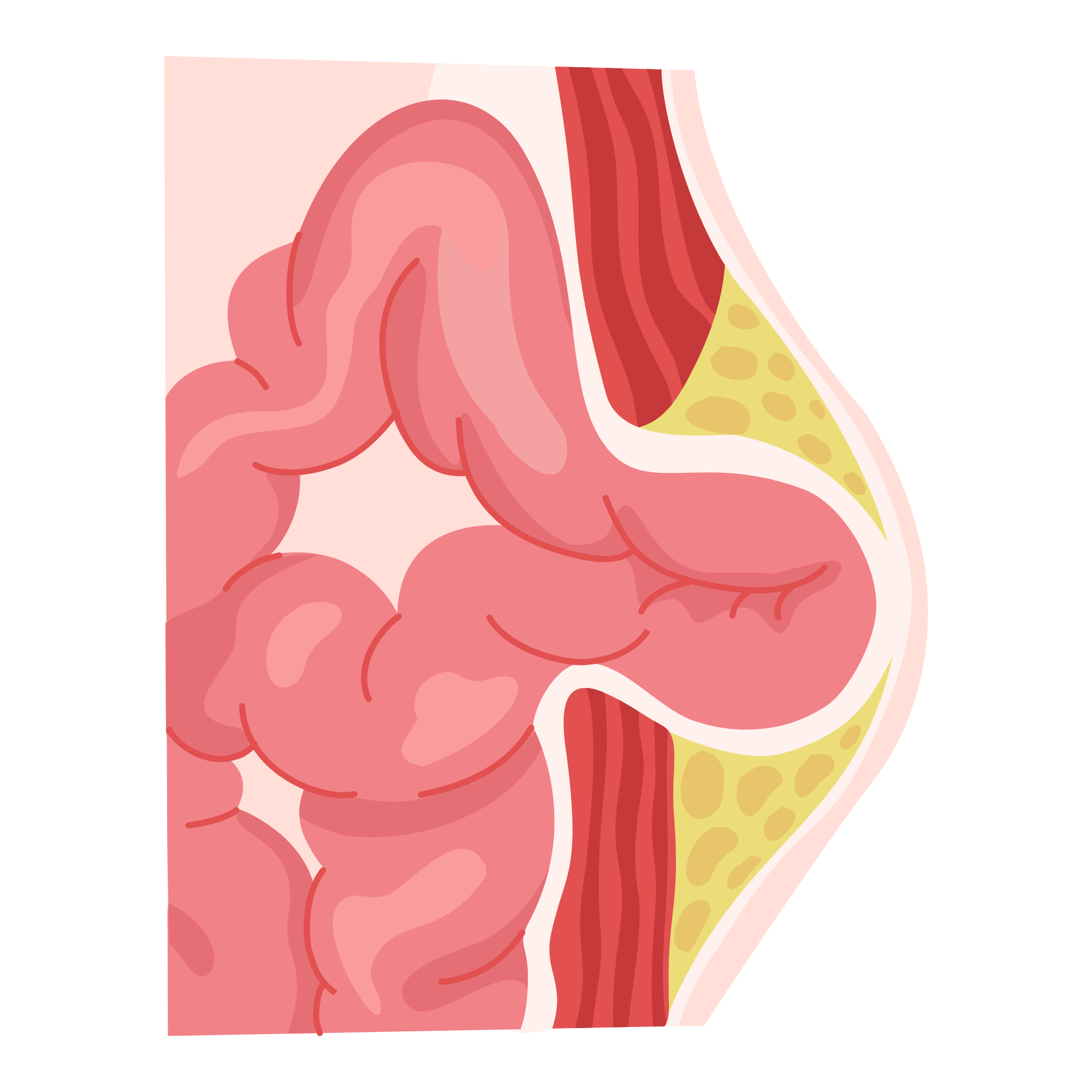 Hernia Repair
Hernia Repair Hysterectomy
Hysterectomy Ovarian Cystectomy
Ovarian Cystectomy Tubectomy & Ectopic
Tubectomy & Ectopic Laser Piles
Laser Piles Laser Fissure
Laser Fissure Varicose Veins
Varicose Veins Laser Fistula
Laser Fistula Pilonidal Sinus
Pilonidal Sinus