Minimally invasive uterine removal for fibroids, endometriosis, or gynaecological conditions — with smaller scars, faster recovery, and less blood loss than open surgery.

A hysterectomy is the surgical removal of the uterus. It is recommended when other treatments have not controlled symptoms adequately. The most common reasons include large or symptomatic uterine fibroids, endometriosis causing chronic pelvic pain, abnormal uterine bleeding unresponsive to medical management, uterine prolapse, adenomyosis, and in some cases early gynaecological cancers.
Laparoscopic hysterectomy offers a major advantage over the traditional open approach. With just 3 to 4 small incisions, the surgeon operates through a high-definition camera and specialised instruments. Blood loss is considerably lower, post-operative pain is reduced, and patients leave hospital within 1 to 2 days rather than 4 to 7 days for open surgery.
Depending on the reason for surgery, the ovaries and fallopian tubes may be left intact. When the ovaries are preserved, hormone production continues normally and menopause does not occur prematurely. The appropriate scope of surgery is discussed with each patient based on her age, diagnosis and preferences.
Book a consultation with Dr. Prashanth J V today.
Book Consultation 📞 +91 93533 16175The operation is performed under general anaesthesia and typically takes 60 to 90 minutes. A uterine manipulator is inserted vaginally to allow precise positioning during surgery.
General anaesthesia is administered. A urinary catheter drains the bladder during surgery. The abdomen is prepared and sterile drapes are positioned.
Three to four small incisions (5–12 mm) are made. Carbon dioxide gently inflates the abdominal cavity, creating a safe working space and clear view of the uterus and surrounding structures.
Using HD camera guidance, energy instruments carefully seal and divide the uterine blood supply and supporting ligaments. The bladder is gently mobilised away from the cervix.
The uterus is detached from the vaginal vault and removed through the vagina — no additional abdominal incision needed. The vaginal cuff is then sutured closed laparoscopically.
Port sites are closed with absorbable sutures. Most patients are comfortable and walking by the same evening.
Brief hospital stay. Mild abdominal soreness managed with regular analgesics. Catheter removed on day 1 and most patients are walking by the evening of surgery.
Rest at home with short walks encouraged. Light vaginal spotting for a few days is normal. Avoid heavy lifting, driving and vigorous activity.
Return to desk work and light household activities. Fatigue improves steadily. Avoid intercourse until the vaginal cuff heals fully at 6 weeks.
Full unrestricted activity including exercise and intercourse. A follow-up confirms complete healing. Most women report significant improvement in quality of life.
Extensive experience performing laparoscopic hysterectomies with consistently low complication rates and excellent outcomes for patients.
HD laparoscopy, advanced energy sealing devices and meticulous haemostasis to minimise blood loss and speed up healing.
Every patient receives a thorough pre-operative consultation covering all options, risks and realistic expectations before any decision is made.
 Gallbladder Surgery
Gallbladder Surgery Appendicectomy
Appendicectomy Hernia Repair
Hernia Repair Hysterectomy
Hysterectomy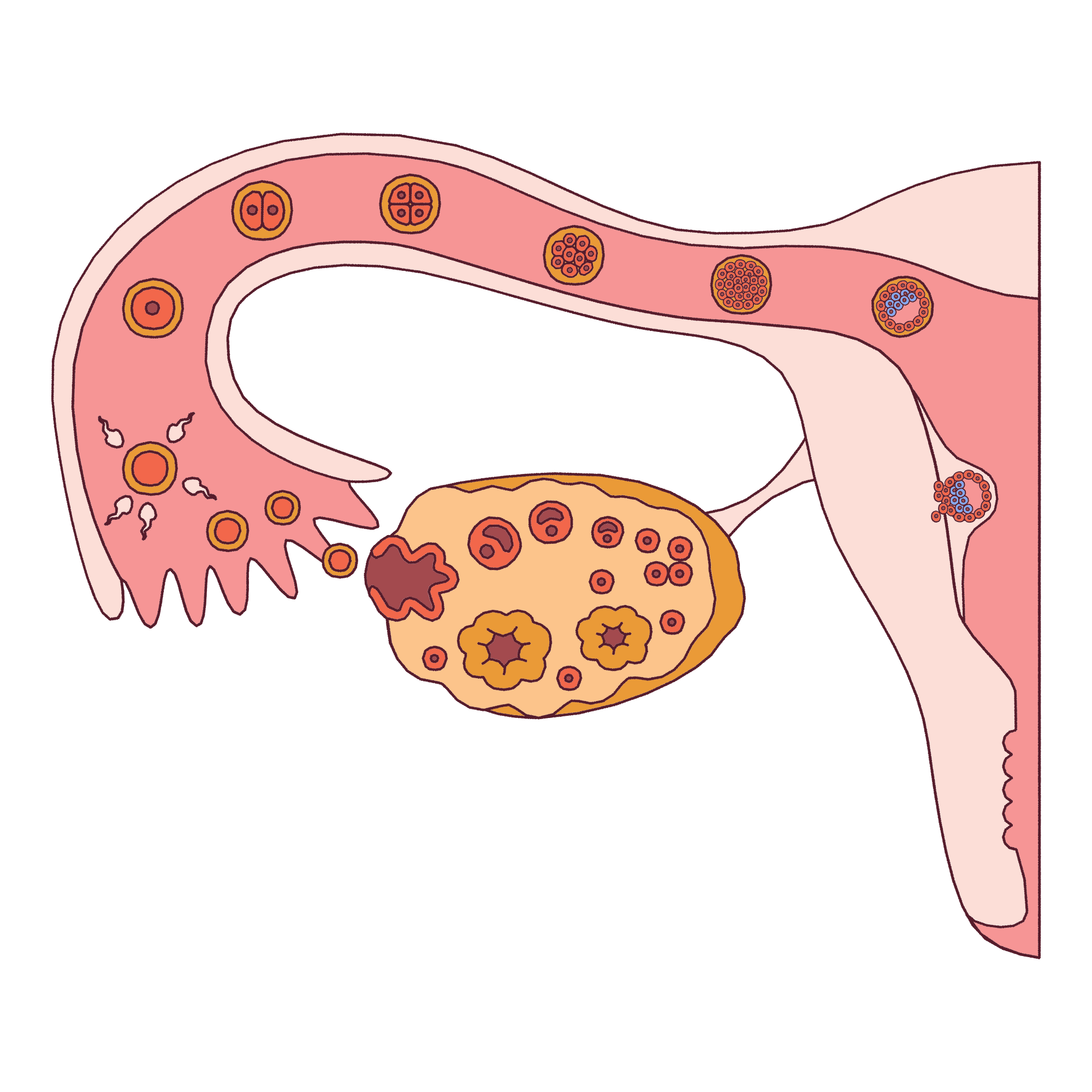 Ovarian Cystectomy
Ovarian Cystectomy Tubectomy & Ectopic
Tubectomy & Ectopic Laser Piles
Laser Piles Laser Fissure
Laser Fissure Varicose Veins
Varicose Veins Laser Fistula
Laser Fistula Pilonidal Sinus
Pilonidal Sinus